Readings in Humanistic Psychiatry
Left-handedness and Disease
This paper will discuss various medical and psychiatric disorders that are found with increased frequency in left-handed people, theories about the causes of these associations, and, especially, what this may tell us about a very important question: What is Schizophrenia?
I’ve been interested in this topic since 1981. At that time I was in my internship, doing a neurology rotation at Sloan-Kettering Hospital in NYC. One day our attending neurologist told us that a Doctor from Harvard named Norman Geschwind was coming to speak with our little treatment team over lunch break. At the time I had no idea that he was someone who would come to be recognized as the father of modern behavioral neurology.
At the time Dr. Geschwind was working on a monumental, three part article on mechanisms of cerebral lateralization- the ways in which our two cerebral hemispheres are organized and coordinated. Every now and again someone explains things in a way that changes the way you see everything. This was clearly such an occasion.
Dr. Geschwind introduced us to the idea that a number of seemingly unrelated disorders are found with increased frequency in left-handed people and discussed his ideas about why this might occur. I don’t recall him ever discussing mental illness per se but, over time, I found that his theories dovetailed nicely with some emerging models of schizophrenia.
Before we proceed, a word of caution: One should always remember that anyone can have a theory about anything. Even psychiatrists who possess slides and diagrams should have their ideas taken with a large grain of salt.
Left-handedness through the ages
The differences between right and left-handers have fascinated humans for centuries. Consider this quote from the Book of Judges:
At once the Benjamites mobilized twenty-six thousand
Swordsmen from their towns, in addition to seven hundred
chosen men from those living in Gibeah. Among all these
soldiers were seven hundred chosen men who were left-handed,
each of whom could sling a stone at a hair and not miss.
Judges 15
One can see that even back then people recognized that left-handers were somehow different. They certainly weren’t as common. Seven hundred out of twenty-six thousand represents only about three per cent of the group. And there is already the idea that lefties may be more talented in certain areas- in this case slinging stones at other people.
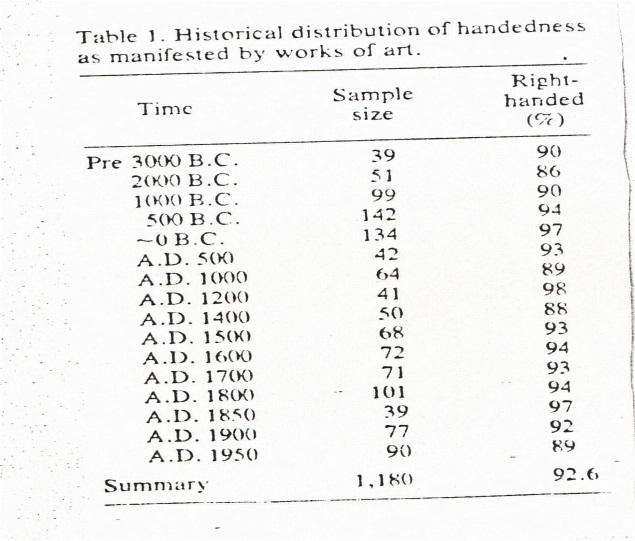
An interesting article in Science looked at over 12,000 ancient paintings and sculptures dating back to 15,000 B.C. and examined them for any evidence of hand-preference. Their conclusion was that humans have always been a predominantly right-handed species. As can be seen in the table below, they found that roughly 93 % of people were portrayed as right-handed. We’ll see later that this is surprisingly close to current estimates of the incidence of right-handedness.
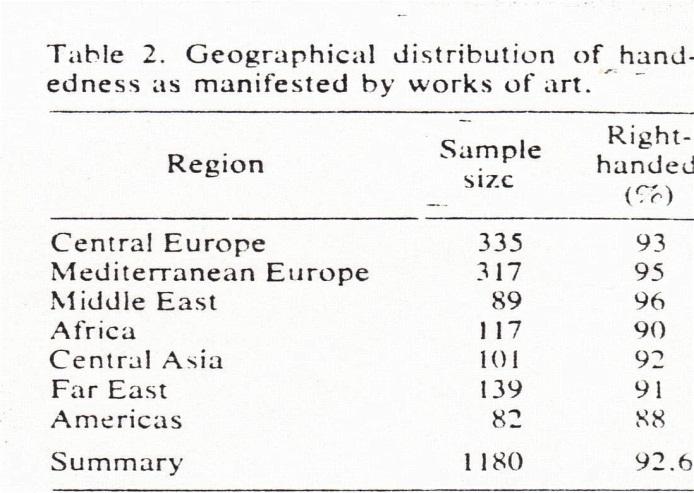
The increased frequency of right-handedness appears to be found consistently around the globe as well:
A recent study of fetal ultrasound data suggests that even in the womb humans are more likely to be right-handed. Babies sucked their right thumbs far more often than their left ones.
What about other primates?

Existing data from primate research confirms that other primates show hand-preference as well, and that their preferences follow a clear pattern. Lemurs and other prosimians tend to be left-handed. As one “ascends” up the evolutionary tree we see that macaques and other old-world monkeys are about equally split between right and left handers.

Among gorillas and chimpanzees about thirty five percent of individuals favor their left hand while in humans that figure hovers pretty close to ten per cent. So in broad-brush terms it seems that the more “primitive” the primate the more statistically likely it is to be left-handed. So, in evolutionary terms, left-handedness seems to predate right-handedness.
While many of us now accept the idea that differences in handedness must be related to underlying differences in the structure of our two cerebral hemispheres, that turns out to be a pretty recent idea. As recently as the mid nineteenth century people believed that our hemispheres were no different that our eyes, lungs, kidneys, or any other of the paired organs. We assumed that they’d be identical in structure and functioning. So the ideas of Brocha and others that suggested that specific functions could be located in different cerebral hemispheres were quite revolutionary at the time.
Difficulties in understanding handedness research in humans
Like it or not, we’re prone to biases when we try to examine the assumption that there might be differences bewteen right and left-handed people. Some of them can be found in the very terms that we use for our hands.
In our culture, we refer to the “right” hand. Of course “right” also means proper or customary. In the sciences we sometimes use the word “dextral” when referring to the right hand. If someone is particularly skilled at a task we might say that they have “dexterity” or “adroitness” – other words that have roots in right-handedness.
The word “left” is derived from the Old English “lyft”- a word that historically meant weak or useless. In Latin the word for left is “sinister”. In the sciences left-handedness is sometimes termed “sinisteralism”. So we must deal with ancient ideas that left-handedness reflects “the hand of the devil”. For many centuries, across a variety of cultures, there have been efforts to convert left-handed people to righties, as though there was something inherently wrong with being left-handed.
Because of these myths and prejudices there is still a lot of skepticism about the notion that left-handers are really different than right-handers in any important ways. The belief that “all men are created equal" has morphed into the politically correct idea that all humans are exactly the same.
In the last few decades there have been a number of studies on the topic of handedness and we’ll try to review a few of them here. But as soon as one turns to the literature some significant obstacles are encountered. One is simply that it’s a huge topic. Another lies in the difficulties with reliably assessing handedness. Research historically determined handedness in the simplest of ways: “Which hand do you write with?” was sufficient to classify people into two broad groups.
In the current literature handedness is now seen as a continuous variable, much like one’s height. People are seen as occupying a point on a spectrum of handedness preferences. You’ll see the term “ non-right-handedness” which refers to anyone except people that are strongly right-handed. “Mixed –handedness” refers to people that typically use different hands for different tasks, i.e. someone who writes with one hand but eats with the other.
“Ambiguous handedness” captures people who might use one hand for a given task at one time but use the other hand the next, as though there is no clear preference for handedness at all.
And even among left-handers there are now efforts to tease out people that are right-brain dominant for speech ( about 15 % of lefties ) versus ones that have the more typical left-brain speech centers.
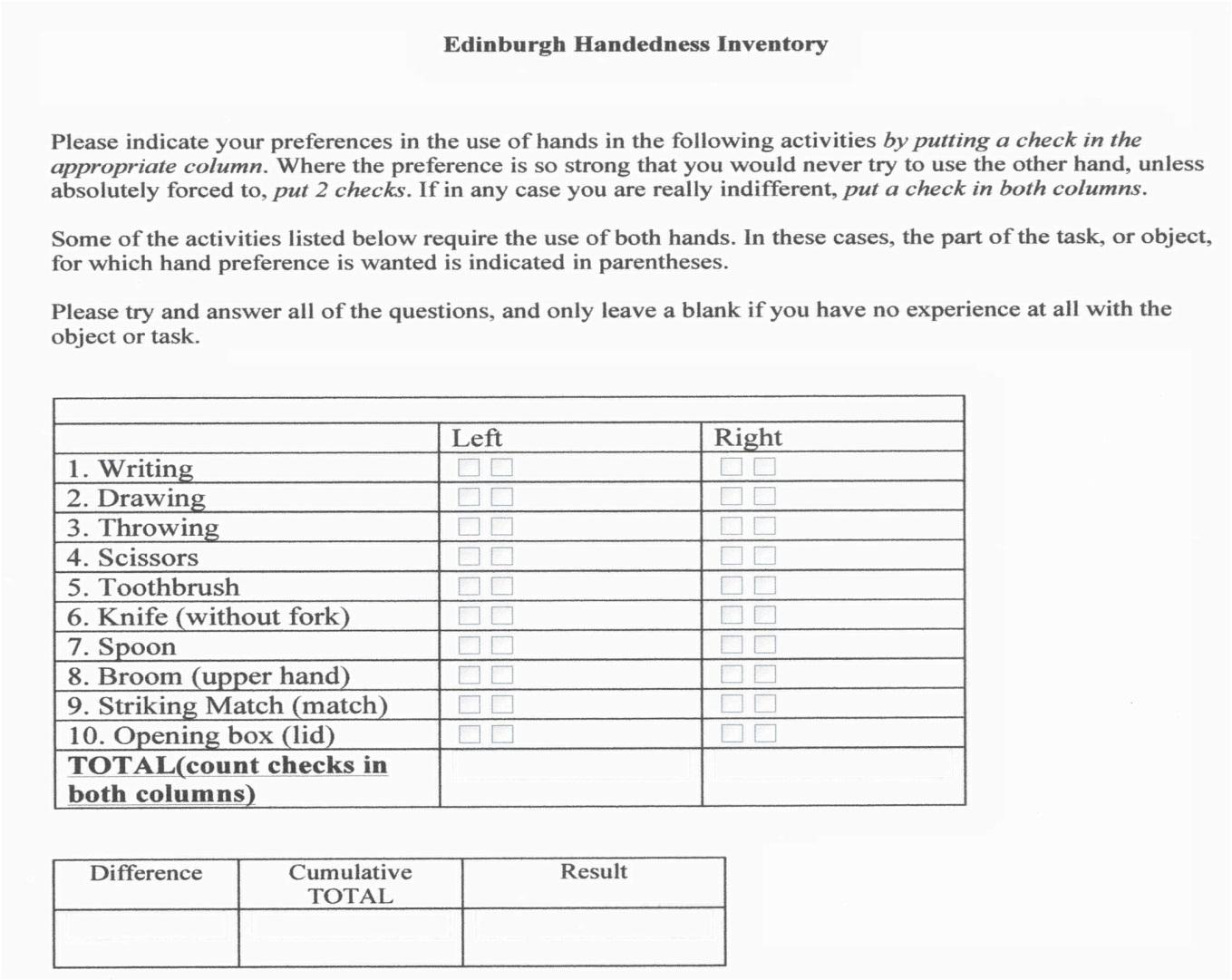
So research instruments have now progressed from the simple question about writing to evaluation of a series of common activities. The scale pictured above is one that’s commonly used in handedness research but there are far more complex and detailed versions available. Most end up creating a minus 100 to plus 100 scale, with one end representing a total preference for the left hand and other other for total right-handedness. Most people fall somewhere between the extremes.
When assessing handedness research we must also take into account the age of the subjects. Handedness is generally thought to establish itself around the age of five or six, with females often “declaring” their hand preference a bit earlier than males. But a tendency towards right-handedness can increase over time and some people even switch functions to their right hand into their thirties.
When all of the studies are in it looks like the incidence of left-handedness runs right around 7-10 % in humans.
Associations between left-handedness and various medical conditions
It’s difficult to study the incidence of relatively rare disorders using small groups of people. In an ideal research world when one wants to study whether a particular disease is found with increased frequency in one handedness group compared to another we'd have very large samples of righties and lefties- say at least 100,000 of each- and see how many of each group suffer from the disorder in question. Of course, those sorts of studies are very rarely done.
A more common approach is to look at perhaps 50 or 100 people with a given disorder, say autism for example, and then see if there is more non-right-handedness than statistically expected. We’ll see that some pretty consistent trends do emerge even with the more limited approaches. But first,another word of caution is necessary.
It would be a mistake to conclude that left-handers as individuals are at a disadvantage either medically or psychologically. We’ll see that this is clearly not the case. In fact surprising trends in the opposite direction are encountered.
It’s not a shock to find that many of the first disorders that were found to be associated with increased rates of left-handedness were neurological disorders. When practitioners of different specialities are followed around it becomes clear that neurologists inquire about handedness far more often than anyone else. So seizure disorders were among the first medical problems to be found with increased frequency in lefties. Studies dating back to the 1950s found rates of seizure disorders to be increased two to three fold in left-handed people compared with righties.
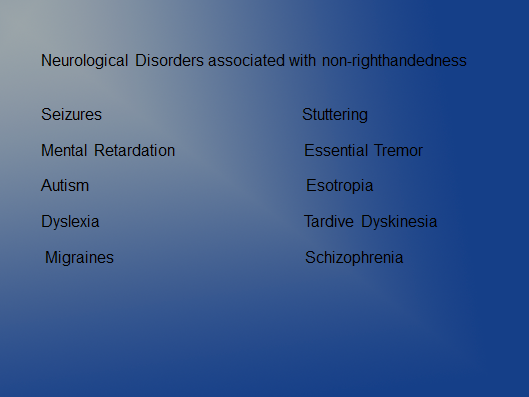
Non-righthandedness has been found with increased frequency in intellectually disabled people. A 20-28 % incidence of what used to be termed “mental retardation” was common in lefthanders and the correlation increased the more severely “retarded” the individual was.
A study of autistic people found that about 18 % were left-handed and a surprising 41% were ambigiously handed.
Dyslexia is another disorder with a strong association to left-handedness. An increased rate of around 15 times that of right-handed people has been documented.
Geschwind himself estimated that stuttering is about five times more common in left-handed people.
So, as the slide above suggests, left-handedness ( or non-righthandedness ) are associated with increased risk of a wide variety of neurological problems. That’s a pretty impressive list but things become even more puzzling when one looks at the incidence of immune disorders.
Left –handedness is found with increased frequency in Crohn’s Disease, Ulcerative Colitis, Celiac Disease, autoimmune thyroid disorders, myasthenia gravis, asthma, hay fever, and exzema. People with cleft lip and palate are about two and a half times more likely to be lefties. Alcoholics are significantly more likely to be left-handed and at least two studies have found their treatment outcomes to be less favorable. Sons of left-handed alcoholics have a poorer prognosis.
Even “normal college students” ( to the extent that they exist ) are found to be about three times more likely to struggle with insomnia if they’re left-handed.
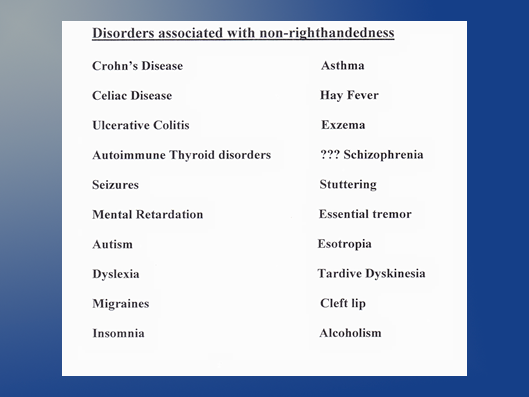
So, as this summary slide suggests, a bewildering assortment of disorders appear to be related to hand preference. Even if one were to arbitrarily drop half of these maladies, attributing them to sampling error or poor study design or whatever, a person would still be hard-pressed to explain the remainder of these associations. Something powerful and important must be going on here.
Left-handedness and increased talents
To make matters even more confusing, left-handedness has been found to be associated with a tendency towards increased talents in a variety of different fields.
One study looked at extremely precocious elementary school students- the top 1 in 10,000 in math or verbal reasoning scores. Only 23 % of these super-bright youngsters were strongly right-handed. The rest were either lefties or mixed-handers.
People with the sorts of talents that many of us envy every day- musicians, engineers, architects are more likely to be non-righthanded.
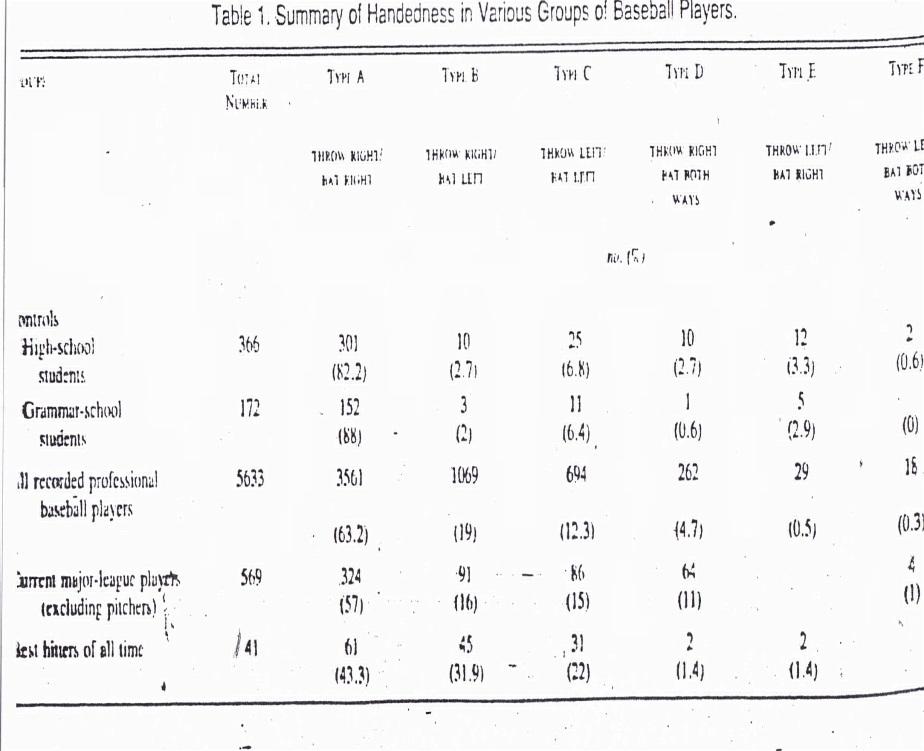
Even more importantly, professional baseball players are more likely to be left or mixed-handed. This is a very poor quality slide from the New England Journal of Medicine, created back in the 1980s when my slides were even more primitive than those I use today. But you can see the basic point. When kids are starting out their baseball careers, in elementary and high school, the rate of left-handedness is about the same as one finds in the general population. But the farther up the baseball ladder one travels, the more likely it is that any given player will be a lefty or mixed-hander. Now some might argue that the left-handed batter’s box is a step closer to first base, or that left-handed hitters have an advantage because they more commonly bat against right-handed pitchers. Both are true, of course. But the increased association between advanced baseball skills holds true for players that bat right-handed and throw left-handed.
The basic idea is that left-handed people tend to be more ambidextrous than strong right-handers. Left-handed people in general are much more coordinated when using their non-dominant side. Many strongly right-handed people basically carry their left arm around without being able to use it for much.
Left-handed bodies appear to be better balanced. Even their fingerprints are less asymmetrical. So a broad overview would suggest that in human evolution left-handedness is sort of an experiment. If you want to build the reliable drone model that’s the strongly right-handed one. Left-handedness can be a tremendous success but there’s a lot that can go wrong when you stray away from the strongly right-handed model too.
So what did that Geschwind guy think was going on?
If anyone is still following along with all this they’re likely to have some basic questions:
What mechanisms could possibly explain this weird connection between handedness, diseases, and special talents?
And what relevance could any of this have to our understanding of schizophrenia?
Most people would agree that just being left-handed in itself would be unlikely to cause all of these correlations.
Even more unlikely would be the idea that all of these separate disorders can somehow cause a person to be left-handed.
These days, a clever scientist might immediately wonder whether there is a special gene for handedness, one that’s located on the same chromosome as genes that cause that wide array of different disorders. There might be something to that.
When two right-handed parents reproduce roughly 2-5 % of their kids will be left-handed. When two left-handed people mate about 35 % of their offspring will be left-handed. So genetics are clearly involved at some level.
Back in the 1970s a researcher named Annett developed what was called the “random dominance theory” of handedness. The basic idea was that there would be a single dominant gene for right-handedness. If it was on one or both chromosomes that the baby inherited then speech would be lateralized to the left hemisphere and the child would be right-handed. If the dominant gene wasn’t present then speech would be randomly distributed between the right and left hemispheres, with motor function following along. The idea has tremendous intuitive appeal and maybe someday that gene will be found. But, so far, a dominant gene for right-handedness hasn’t been located.
This paper was published back in 2007. It implicates a gene for handedness called “leucine rich repeat transmembrane neuronal 1- LRRTM1”. The idea is that when the gene is present and fully activated it causes a person to be left-handed. The gene appears to be transmitted by the father and is usually suppressed or turned down in females. It also contributes to the formation of brain areas involved with speech and emotion. And it seems to be on the same chromosome as another gene that has been implicated in schizophrenia.
But it’s looking like there’s a lot more to the story than the actions of a single gene.
Back in the early 1970s a theoretician named Paul Satz proposed the concept of what he termed “pathological left-handedness”. The basic idea was that some sort of developmental insult harmed the brain’s left hemisphere during fetal development. As a result, some functions were shifted to the right hemisphere, including hand preference.
He thought that as a result of that shifting of functions there was a “crowding effect”. So when there were too many functions located in the right hemisphere things just weren’t likely to work as well. He did present some pretty convincing evidence that early brain damage is associated with an increase in left-handedness.
Satz’s ideas about there being different causes of left-handedness and early damage to the developing left-hemisphere being one of the significant causes were useful. But that would not explain things like the association between left-handedness and immune disorders, those special talents, or oddball phenomenon like the “idiot savant” syndrome that is sometimes encountered in autistic disorders.
That’s where Geschwind’s work comes in.
In 1985 Norma Geschwind and Albert Galaburda published their theory of brain lateralization in the Archives of Neurology. It’s a monumental, three part article and I couldn’t do justice to it even if I were capable of understanding it. But there were several basic assumptions that are worth reviewing:
They believed that the basic pattern for the human nervous system is one that favors left hemisphere dominance for speech and motor function ( remember that the left hemisphere controls the right side of the body and vice versa ).
They believed that the common asymmetry of functions must be rooted in an asymmetry of brain structures.
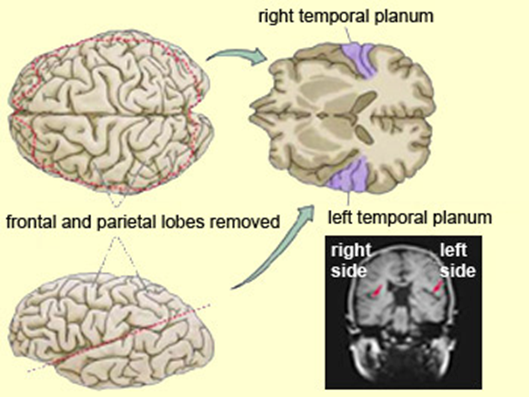
They noted that there is an area in the posterior portion of the left temporal lobe, the left planum temporale, that is typically larger than its counterpart on the right side. They found this association to hold among fetuses, newborns, and adults. When they examined fossilized human skulls they concluded that this has been true for many centuries.
Geschwind and Galiburda also stressed the fact that in human fetuses the right hemisphere actually develops more rapidly than the left one. So the left hemisphere is vulnerable to changes in the intrauterine environment for a longer time than the right side is. If there were some sort of insult to the fetus’s development it will hit the two hemispheres at different stages of development. And the left planum temorale is the last cortical area to complete neuronal migration and hook-up so it seems to be the most vulnerable area of all.
Their belief was that some influence in the intrauterine hormonal environment interferes with, or delays, the maturation of the left hemisphere. They figured that the hormones that the fetus is exposed to are the most likely culprits. And they suspected that testosterone was the main player when determining brain lateralization.
Today we well know that testosterone has a lot to do with how we build our brains. Many of us have been quite disappointed to learn that the basic structure of the human nervous system is a female one. When testosterone is around in sufficient quantities the brain is changed pretty dramatically. Humans have important brain nuclei that are “sexually dimorphic”. They’re of much different size in men compared to women and it looks like the amount of circulating testosterone in the fetal circulation is responsible for the differences.
It may come as no surprise to some that when there is a lot of testosterone present during fetal development the areas of the brain involved with social skills and communication don’t develop as well. On the other hand, important brain areas that allow us to orient ourselves in space and recognize patterns become larger. The idea is that these changes in brain structure and functioning date back to our hunter-gatherer ancestors.
In hunter-gatherer societies the hunter males had to be quiet while they stalked their prey. Being able to find their way back to the cave or settlement was of crucial importance. So some of the brain areas associated with those functions ( parhippocampal gyrus being a good example ) enlarged and became more functional. Females tended to stay closer to home, in the company of other females. They could chatter together all day and if they talking stopped that was likely a bad sign. Obviously, these basic differences between the genders are still with us today and they must have their origins in the different structuring of our brains.
Another of Geschwind’s basic assumptions was the idea that if something interferes with the construction of one of the cerebral hemispheres, the corresponding area on the other side is likely to become enlarged and increase its functioning. So if the left hemisphere’s development is delayed or it’s exposed to a hormonal insult the right hemisphere may become overdeveloped, in some cases to an extent where it becomes dominant for speech or hand preference even when the genetics don’t call for that.
They called this increased right hemisphere functioning “the pathology of superiority” and they thought that it may explain some of the increased talents often found in left-handed people. They even speculated that this could be the explanation for the “idiot savant syndrome” associated with autistic disorders. The idea was that left hemisphere mal-development caused the core problems with speech, language, and social skills in autistic people but sometimes little pockets of brain on the other side enlarged and became hyper-connected. How else can we understand situations where kids that can barely communicate can somehow recall an entire symphony after one playing, or tell what day of the week June 16th will fall upon in the year 3033?
So Geschwind saw atypical handedness as a potential marker for problems in neurodevelopment. And he believed that the same factors that were influencing the development of the left hemisphere during fetal life might also affect the development of other organs or structures that were developing at the same time.
He particularly emphasized the effects of testosterone on the developing thymus and believed that was at the heart of the problems with immune system development that often coexist with the altered brain lateralization.
He took note of the fact that boys tend to have more allergies than girls during childhood but with the onset of puberty- with its increased testosterone levels- males often “outgrow” their allergies. Women tend to suffer from more autoimmune disorders than men- but only until the male’s testosterone levels drop later in life. In our later years we males tend to have autoimmune problems at about the same rate as females do.
Geschwind died in 1984, before this enormous work was published. Before he passed, he acknowledged that his theory was crude, and that it would have to undergo significant modifications even if it were proven correct. But he believed that the one thing that was indisputable was that there is an intimate relationship between intrauterine sex hormones, the development of our immune systems, and the way that we humans lateralize our brains.
He also emphasized that it might be sensitivity to circulating hormones that was important- not just whether levels of one or another were high or low.
We’ve since gone on to learn that the hormonal environment that the fetus develops in does have a huge impact on the way that the brain is ultimately structured.
All of these hormones are now recognized as major contributors to fetal brain development. We’ll be sorting out which hormones affect which brain structures in what ways for decades to come. But that basic idea that babies build their brains in response to the environments that they- and indirectly their mothers- are exposed to, and that those intrauterine hormones are the primary mediator of that, now seems pretty certain.
Schizophrenia and handedness
It wasn’t that long ago that schizophrenia was felt to be a “functional brain disorder.” The assumption was that the brains of people who suffered from this illness were basically structured normally but they just weren’t working properly for some reason.

For a while it was taken as a given that the real cause of schizophrenia was bad mothering. The concept of the “schizophrenogenic mother” is still a cause of bitterness for some parents that were unfortunate to have been exposed to it.
Later, of course, we entered into the “chemical imbalance model” of schizophrenia. We still are influenced by its basic assumption- that there must be some imbalance of brain chemicals – neurotransmitters- that is responsible for the characteristic hallucinations, delusions, and disorganization found in the disorder.
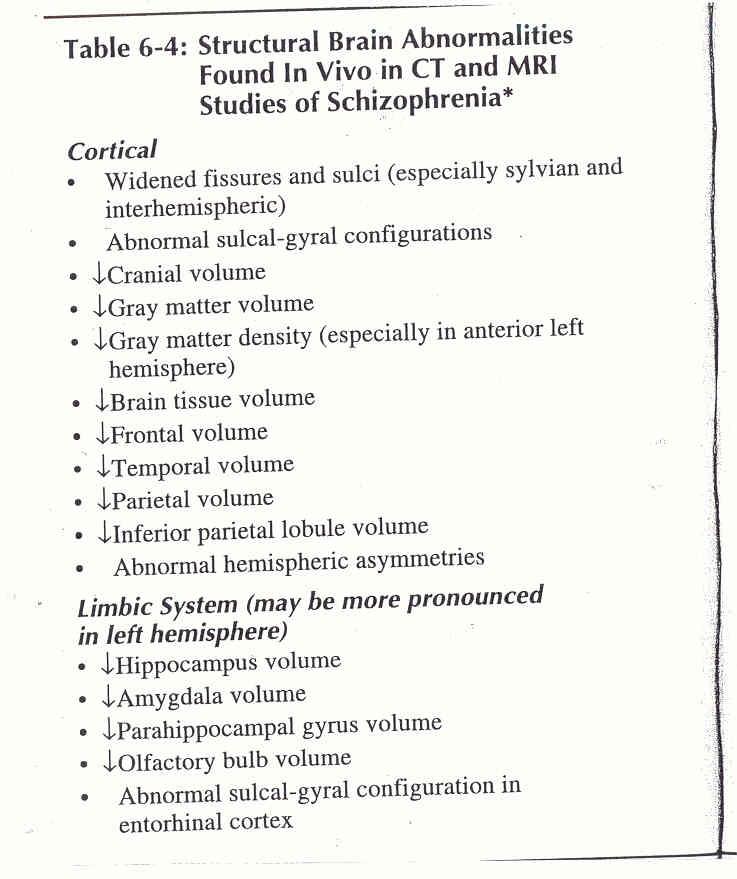
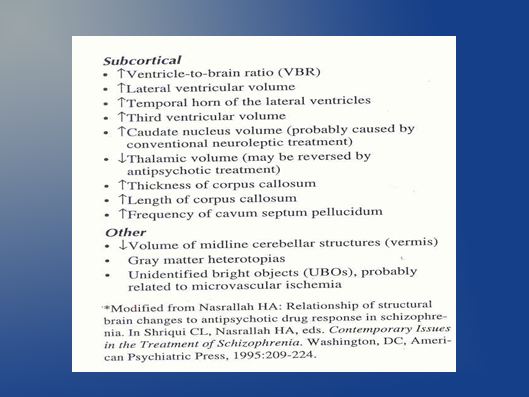
Now days it would be hard to find a serious neuroscientist who believes that schizophrenia is the result of something as simple as one of those “chemical imbalances”. This is an old and very incomplete list of brain structures that weren’t properly formed and connected in the brains of people with schizophrenia during fetal development. That increased length and thickness of the corpus callosum is of particular interest as that’s a major route on communication between the brain’s two hemispheres.
We’ve known for some time now that the “concordance rate” for schizophrenia in identical twins is about 50%. This certainly speaks to the importance of genetic factors in the illness but, at the same time, argues for something else going on as well. For if schizophrenia were purely a genetic disorder we’d expect that two identical twins- with exactly the same genetic complements- would always have the same rates of the illness.
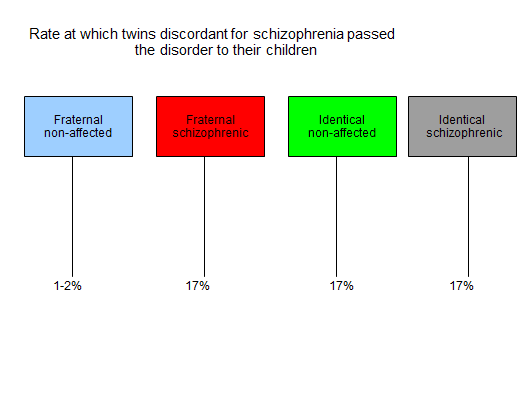
This slide shows a surprising finding that came out of long-term studies of schizophrenia in Denmark. The shocker was that the identical twins discordant for schizophrenia ( one had it, the other didn’t ) passed down schizophrenia to their children at the same rate. This led to what has been called the “second strike hypothesis”- the idea that genes are very important in creating the disorder but that in many cases something else has to happen, the second strike, for the illness to develop in its full form.
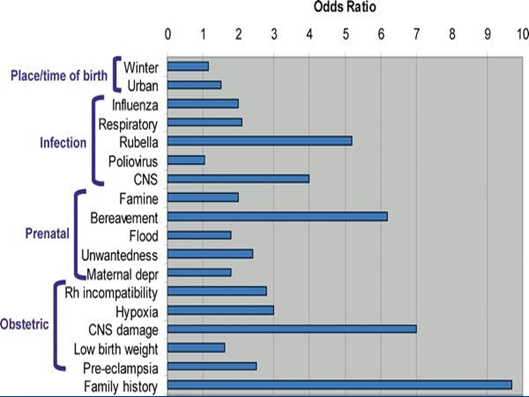
We’ve now gone on to identify what some of those “second strikes” might be for any given individual. The table below contains some factors that are intuitively obvious (e.g. obstetrical complications, infections, etc ). Some ( e.g. winter birth, urban environment ) have been recognized for many years. But for some of us, this list would be extremely hard to explain away with implicating those changes in circulating maternal hormones that Geschwind thought to be so crucial for brain development. How else can we directly tie the mother’s emotional state due to flood, famine, loss of a loved one, or not wanting the child to the baby’s eventual brain structure and functioning? Any competing theory of schizophrenia will have to establish a different mechanism for how each of these risk factors would operate.
Schizophrenia has been associated with an increased rate of left and mixed handedness for many years. There are now suggestions that non-righthanded individuals may have a more severe form of the disorder, with more prominent deficits showing up on neuropsychological testing batteries.
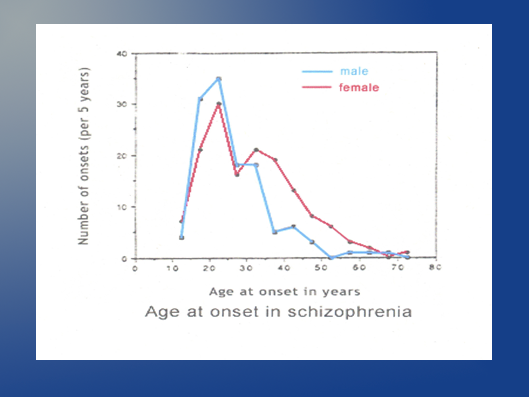
Any comprehensive theory of schizophrenia will also have to account for some other unusual features of the disorder: The full syndrome typically doesn’t emerge until late adolescence or early adulthood, sometimes even later. And the illness tends to behave differently in females than in males. Males typically have an earlier onset of illness and more severe associated cognitive problems. The ultra-late onset cases, those arising in the 40’s or even into the 50’s are almost always females. In diagnostic manuals prior to the current DSM 5 the majority of these late-onset cases qualified for a “Paranoid Type” diagnosis but the subtypes of schizophrenia were not used uniformly and have now been eliminated.
As can be seen, this implied that the individuals did not show prominent disorganization of speech or behavior, flat or inappropriate affect, or catatonia. Many researchers suspect that this may actually be a different illness than other types of schizophrenia.
Schizophrenia as a neurodevelopmental disorder of brain lateralization
So it does seem possible that schizophrenia is somehow related to changes in intrauterine sex hormones and the ways that they affect brain lateralization. But if that’s true, what mechanisms might be involved?
We’ve already looked at the idea that sex hormones could have direct effects on how the brain is structured- on the very nerve cell migration and hook up that goes on during fetal life. But there may be more involved than that.
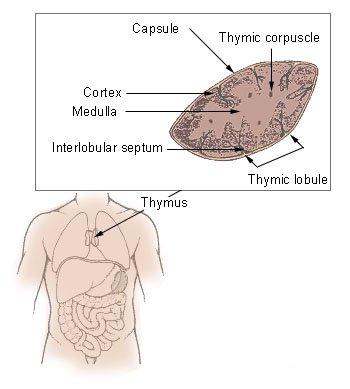
Let’s return to Geschwind’s ideas about the role of the thymus. This strange gland is involved in the development of immune processes. It builds the T lymphocytes that we use to recognize antigens on the surfaces of cells- which allows us to decide whether those cells are a part of us or are indicative of the presence of foreign invaders. We know that the body does not always guess right on that question and there are numerous examples of our bodies attacking our own cells by mistake.
And we’ve also learned that the thymus is highly sensitive to the effects of circulating sex hormones, especially testosterone. This gland grows in size from birth until puberty. When the sex hormones begin to increase the thymus shrinks. In adulthood it atrophies and its active cells are replaced by fat – unless the person is unfortunate enough to be castrated. If there are no sex hormones around the thymus becomes large and active again.
One might ask “ So what?”
But consider this curious fact: Our adult brains contain on the order of one hundred billion neurons. In weeks 15 to 20 of fetal development we go through a stage where we produce 250,000 new cortical neurons per minute. Each one of those neurons has to migrate through layers of other neurons to reach its final position and compete for neuronal connections with other neurons. One neuron may create synaptic connections with as many as a quarter million other neurons. But what guides this process?
We humans only have about 35, 000 genes. So there’s no way we could have enough genetic instructions to tell each one of those billions of neurons where to migrate to and who to hook up with. So perhaps immune mechanisms are involved. The neurons recognize each other by the antigens that exist on their cellular surface. Of course, that would depend on intact, well-functioning immune systems. If there are problems with the antigenic tagging and recognition process weird things can happen. Cells might not recognize each other . They might not migrate to the right area or connect with the proper neighbors.
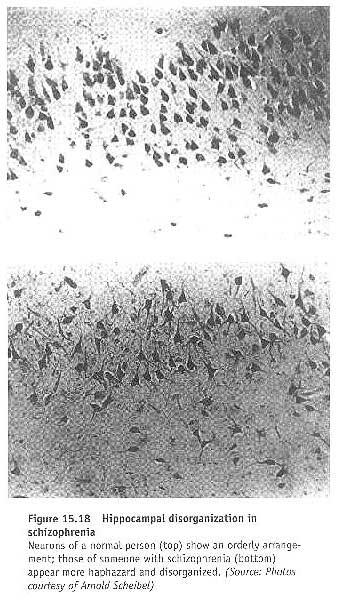
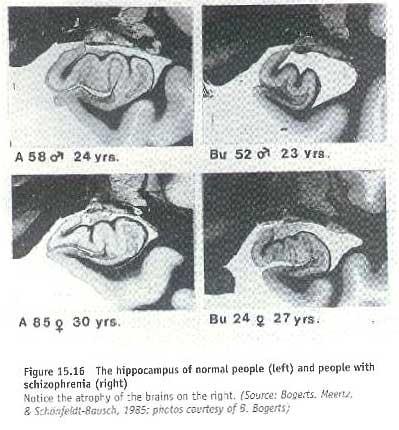
This certainly seems to be the case in a brain area that’s been implicated in all of the major mental illnesses- the hippocampus.
And autoimmunity can develop- where cells recognize our own tissues as foreign invaders and attack them. This mechanism is involved in Lupus, Type I Diabetes, Rheumatoid Arthritis, and a wide variety of other illnesses.
And low and behold, the Danish Schizophrenia registry found that having an autoimmune disease- any of them- increases one’s risk of having schizophrenia by 45 %.
This sets the stage for several interesting theories about schizophrenic illnesses.
Feinberg
One of the puzzling things about schizophrenia is that the characteristic symptoms typically show up in late adolescence or early adulthood rather than being present from birth. Some studies have actually started to challenge that notion and find that some subtle differences in social and physical coordination may be present during early childhood. But few would disagree that the delusions, hallucinations, and disorganization of speech and behavior don’t usually appear until later on. The fact that the illness presents differently in men versus women, with a trend towards later onset in women, would also intuitively support the idea that hormonal differences might be at work.
As can be seen above, in 1983 a sleep researcher named Feinberg proposed the theory that the human brain undergoes a profound reorganization of structure and function during adolescence. He believed that the basis for this lay in the programmed elimination of synapses.
The basic idea was that we build big, fuzzy, hyper-connected brains during childhood. Then as we approach adulthood we develop our adult brains by “pruning” away connections that aren’t needed. So we “tune” our brains to our environments based upon the circuits that we use a lot as we interact with external reality. As our nervous systems are streamlined our adult cognitive processing appears and our problem solving power begins to grow.
It would be hard to imagine how we could recognize and eliminate various neural elements without using our immune systems to carry out the tasks. And this brings us to a crucial idea: that structures built in an abnormal immune environment are more likely to be subject to immune attack later on.
So maybe when the brain undergoes this dramatic reorganization- and decides which neural elements should be kept and strengthened and which should be eliminated- something goes wrong.
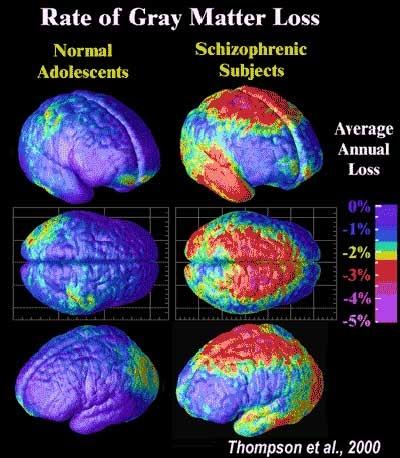
We now know that adolescents who will eventually develop schizophrenia lose gray matter at a much greater rate than “normal” kids. This is scary stuff. Using a computer analogy this gray matter loss is akin to losing processing power.
So it does seem that Feinberg’s theory may provide a possible link between changes in the immune system in utero and later brain changes that might underlie the onset of schizophrenic illness.
Nasrallah
Not too long after Feinberg published his work on synaptic pruning, a psychiatrist named Henry Nasrallah and his colleagues published a fascinating theoretical article titled “ The unintegrated right cerebral hemispheric consciousness as alien intruder: A possible mechanism for Schneiderian delusions in schizophrenia”. Reference below.

The basic idea here is that each of our two cerebral hemispheres produces its own view of the world, then these two world views have to be neurologically integrated into a seamless whole.

It’s been accepted for a long time now that each of our hemispheres has its own areas of strengths and talents. As can be seen above, the left hemisphere typically is more logical, sees things in sequences, uses words as symbols, and has a sense of time. The right produces a more broad-brush, intuitive view of reality. It doesn’t see things in terms of time or sequences and is more intuitive than rational.
While we usually call the left hemisphere the “dominant” one it could be argued that in the course of human evolution, especially prior to the development of language, the right hemisphere may have been the more crucial one. This may explain why the brain develops the right hemisphere more quickly than the left in the majority of cases.
Studies with people who have had their hemispheres surgically separated, or who have one hemisphere put to sleep by injections into its carotid artery, show that the differences in our hemispheres are much stranger than we’d originally thought however. In very real ways it is like we have two separate consciousnesses cohabiting our skulls.
Each hemisphere might have its own emotional outlooks on the world, its own political opinions, and own moral views. The left tends to see things in a more happy, optimistic light. The right’s view of the world is more dark and gloomy.
So Nasrallah suggested that maybe there is something wrong with the way our two world views are integrated, for we should never have awareness that there are two separate views of reality being created in our heads at the same time. That could get a bit distracting.
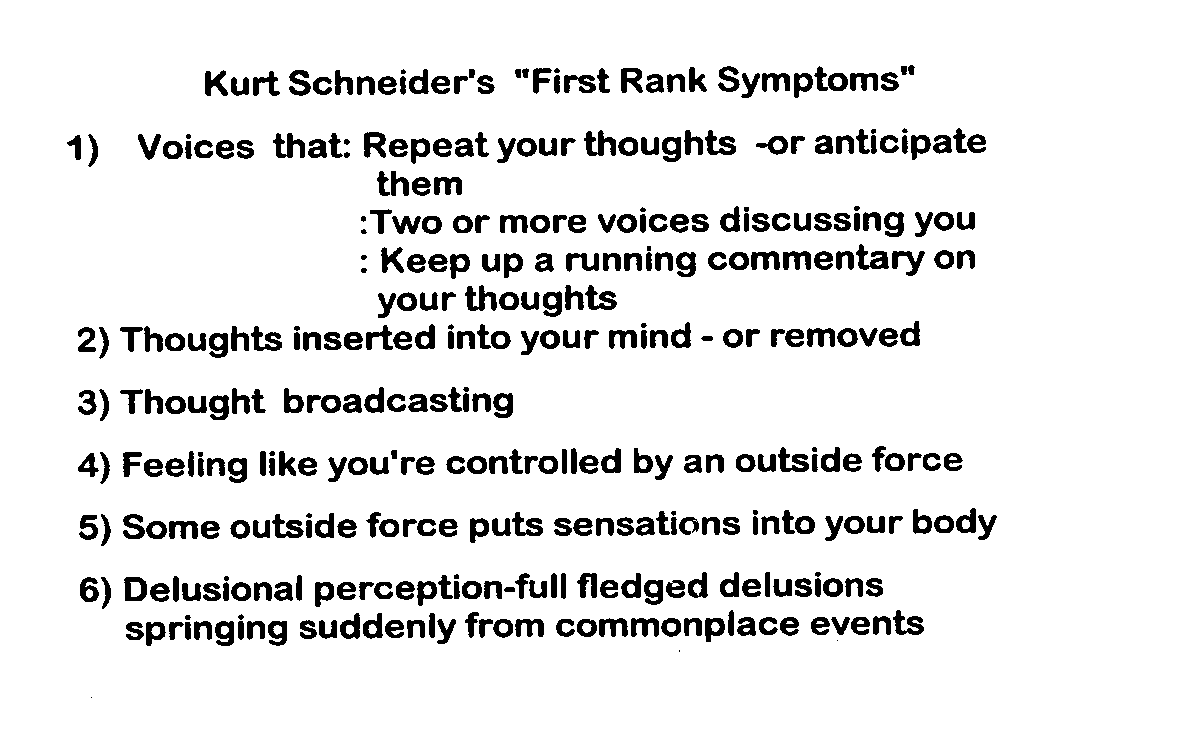
When Nasrallah referred to “Schneiderian” symptoms in schizophrenia it was these classic symptoms that he was referencing. They were first elaborated by a German psychiatrist named Kurt Schneider in the 1950’s and still serve as the basic for our diagnostic approach to schizophrenia today. One might also hear the term “First Rank Symptoms” applied to them.
It doesn’t require too great an intuitive leap to think that maybe the experience of hearing voices, or being controlled or monitored by outside forces, are the result of a problem in balancing those two hemispheric views of reality. Perhaps we have a basic neurologic problem in integrating the contents of our two hemispheres and everything else is just an attempt to explain why this bleed through of non-dominant hemispheric consciousness into the greater picture of reality is occurring.
Psychiatrists who have been around long enough can testify to the fact that decades ago patients often explained their Schneiderian symptoms as the work of demons, Nazis, or witches. Patients today are much more likely to invoke “computers” , microchips imbedded in their brains, and so on but they’re all trying to understand the same basic types of experiences.
We do know that in people with schizophrenia the corpus collosum- the fibers that connect the two hemispheres- are about 11 % larger than in “normal” people and the pathways are more active.
And studies designed to determine which hemisphere is dominant for speech in an individual suggest that people with schizophrenia don’t typically have a normal dominance pattern, especially when they’re psychotic. Which hemisphere will be “dominant” in creating the picture of reality can be almost random. When they become less symptomatic- usually in response to neuroleptic medications, their pattern of dominance becomes more like that of non-schizophrenic people but rarely returns all the way back to “normal”.
Jaynes
Perhaps the most interesting and compelling attempt to integrate all of this came from a psychologist and cultural anthropologist named Julian Jaynes. He wrote this book in 1975:
Jaynes died in the 1990’s but there is still an active Julian Jaynes society out there and another book came out a few years ago that examined his theories in the light of modern neuroscience.
While justice to his theories can’t be done here, a brief summary can be offered.
Jaynes believed that one of the great mysteries of schizophrenia lies in the fact that it’s present in every corner of the world, at roughly the same rates, despite the fact that it clearly doesn’t provide any reproductive advantage. In fact some 40 % of people with schizophrenia are virgins throughout their lives.
Another of his basic theories was that human consciousness as we now know and experience it was unlikely to have emerged suddenly in its present form.

He couldn’t imagine that one day we were dealing with brains like that of our bonobo friend pictured above and the next day we were creating language, books, and architecture.
He believed that there must have been some intermediate types of consciousness on our evolutionary path.
And he believed that they types of consciousness that our brains were capable of producing were dependent on the ways in which the outputs of our two cerebral hemispheres were integrated.
Jaynes thought that the most important characteristic of modern human consciousness is the fact that we are able to utilize what he termed the “Analog I”. We all have this ability to use our “internal screens”. To imagine ourselves in different places or times, doing different things. It is the presence of this “Analog I” that separates us from other primates and from earlier human relatives.
Let’s look at a simple example of how we use this analog self.
Imagine that you have a very important meeting to attend at work but when you wake up you discover that your young child is vomiting and has a fever. What should you do? We face situations like this all the time. When we do we use our minds in a particular way. We’re likely to generate a number of options, and weigh them out in terms of the possible outcomes of each one.
A person facing this dilemma could call in sick at work and take the child to an urgent care center. This would meet the child’s needs but could cause severe problems in the workplace. And maybe the Doctor will say that the kid just has a virus and that nothing need be done in the way of treatment.
The person could try to get a spouse or family member to care for the child. This would meet the needs of the child and the supervisor at work- but could cause friction with the spouse or Grandma as they’d have to change their own plans. Maybe they’ll be less likely to help in the future if they feel put upon.
We might decide the child is facing a life or death emergency, drop everything, and speed down to the local Emergency Room.
Some people would just drop their child off at day care as though nothing were wrong, hoping that no one complains too much about the risk presented to the other kids.
A few people may opt to bring the child to work and have him stay in the car while the parent does their work. The last two options appear to be growing in popularity these days.
All sorts of approaches to the problem are possible and we can prioritize or rank them based on our values and experience. The “Analog I” allows these mental mechanisms. We can ask” What is the likely outcome if I do this?” “How might the outcome be different if I do that instead?” And these mental mechanisms must be rooted in the ways are brains are able to function- particularly in the unique ability to see the same thing from multiple different perspectives.
Jaynes looked at a lot of anthropological data, including the Bible, The Iliad, cave paintings, religious artifacts, and so on. He reached the rather startling conclusion that the type of consciousness that allowed for the use of this “Analog I “ arose only about 4000 years ago. He noted that before 2000 B.C. or thereabouts we had no words for the concept of “insanity”. He thought that everyone back then had some common characteristics with people we now see as suffering from schizophrenia.
His use of the term “Bicameral Minds” came from the idea that earlier versions of humans had brains in which the hemispheres weren’t integrated in the manner that they are today. Instead, they had a Bicameral- or “ having two parts” version of consciousness. This did not allow for the sorts of approaches to problems in which lists of options were internally generated and compared. Instead, when faced with a new or novel problem we relied on hallucinated instructions.
In the case of a sick child and conflicting needs a Bicameral Mind might hear a voice saying “bring him to the shaman”. The shaman, in turn, would communicate with a God or spirit that might instruct him to give the child a particular herb or to utilize a special healing ritual.
Jaynes believed that at one point in the evolution of human consciousness everyone heard voices in response to new problems. People had their own persona Gods and there were typically whole hierarchies of Gods for the community. He cited Biblical references that suggest that hearing voices was very common- and that people sometimes battled over which voice really represented the “will of God”. And he believed that ancient societies sometimes used idols, with their enlarged eyes and mouths, as ways to trigger these hallucinations.
In Jaynes’ view, when human brains started to evolve out of Bicameralism and become more like the ones we enjoy today, this was experienced as a loss of direct contact with the Gods or spirit world. People turned to oracles or prophets to try to re-experience that sense of receiving instructions from an all-knowing deity.
Jaynes also saw vestiges of this older, Bicameral type of brain functioning throughout our modern world.
It turns out that about half of children endorse having hallucinated playmates. Not just “imaginary” friends but ones that are actually perceived as “real”.
We’ve also learned that hearing voices is a lot more common in “normal” people than we’ve usually thought. Studies suggest that as many as 40 % of non-mentally ill people may have heard voices at a particular time in their life, usually an especially stressful time.

And Jaynes especially thought that schizophrenia was a partial return or throwback to that older type of Bicameral mental functioning. He thought this was why schizophrenic illness is found everywhere and is just part of the human condition. He noted how commonly people with schizophrenia hear voices that instruct their day to day decision making. But nowadays our voices are more likely to be experienced as coming from electrical appliances than stone idols.
Just about everyone who has spent a lot of time with people suffering from schizophrenia has heard the complaint that “I can’t think anymore”. It’s often met with frustration as it’s difficult to imagine that someone’s mind doesn’t work just like our own. We might protest “of course you can think- if you couldn’t we wouldn’t be having this conversation”. The fact that these people are trying to explain a very real change in the way that their minds are working, one that robs them of their ability to manipulate symbols on their inner screens and access the “Analog I” , can be very difficult to truly appreciate.
That tendency to believe that other human’s brains, and their resultant experience of reality, are just like our own can be almost insurmountable. So it’s extremely difficult to imagine that young children today, patients with psychotic disorders, or people that lived in ancient societies might have dramatically different brains- and see the world in very different ways than we do.
Jaynes’ theories seem quite compatible with the other ideas that view schizophrenia as a problem of brain lateralization and the integration of our two hemispheres. So what are the implications of all this?
One immediate question is: “If there’s a problem balancing the outputs of our two hemispheres then what is responsible for the balancing?”
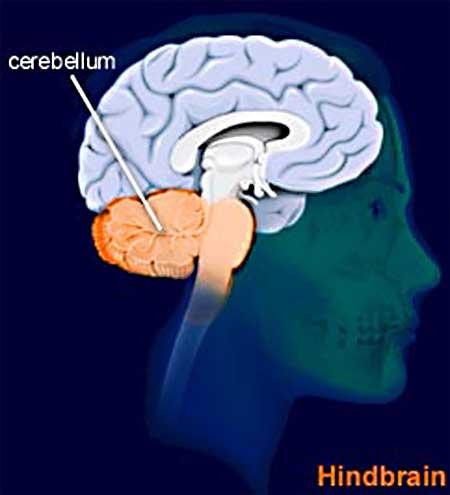
Perhaps in coming decades we’ll see more importance given to the cerebellum as we develop new models of mental illness. After all, this structure contains about half of our brain’s cortical neurons. While it clearly helps to balance our motor movements, our human physical talents don’t explain why we’d devote so much of our brainpower to the cerebellum- or why it is so much larger in human beings relative to the cerebelli of other primates.
Perhaps the more important message found in this work is that recurrent idea that “brains develop and function according to the environments that they develop and function in”.
If it’s true that schizophrenia- and perhaps most of the major mental illnesses- are based in the ways that our brains are structured during fetal life and early childhood, then we can’t expect that simply giving someone a medication will be enough to set them on the path to recovery. Our antipsychotic medications are excellent at relieving some of the positive symptoms of schizophrenia and in most cases they’re an essential element of recovery. But it’s very rare that they restore people suffering from schizophrenia to the condition they’d be in if they didn’t suffer from the illness.
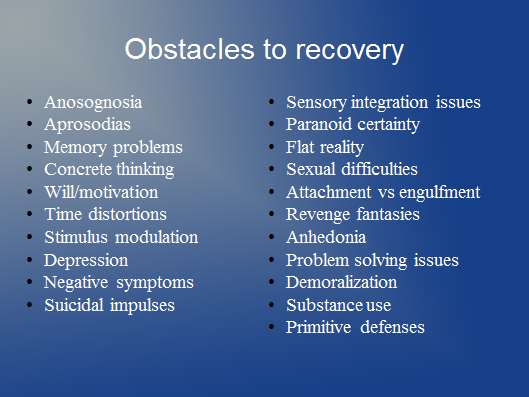
Even when medications work their best individuals still may have to deal with an enormous variety of obstacles to recovery- and each of these potential obstacles can be a deal breaker for any given person.
Unfortunately, our mental health systems themselves can also pose their own obstacles to the recovery efforts of their clientele.
In a more enlightened mental health system we’ll pay more attention to creating the optimal intrauterine environments for our babies to develop in- ones with the right sorts of nutrients, a relative freedom from stress hormones originating in the mother, and the absence of toxic chemicals that might interfere with brain development.
Ideally, we’d spend a lot of our resources ensuring that young children have secure, loving, mentally stimulating environments to grow up in. Making sure that our kids aren’t subjected to emotional, physical, or sexual abuse should become a national priority.
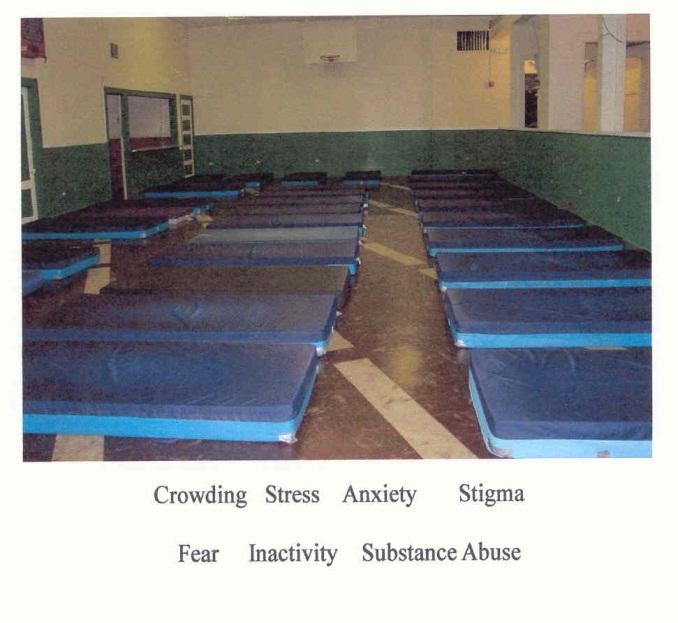
When people do have established severe mental illnesses we’ll want to provide them with living environments that will meet the needs of their nervous systems. We’re already pretty adept at providing them with things that are toxic to optimal brain functioning. So we need to shift our efforts to providing commodities that help any brain to function better.
We should be finding ways to find out exactly what environmental variables are necessary for optimal brain functioning, then revamp our mental health systems to provide those things in the most humane and cost-effective manner possible. Anyone that’s interested in seeing what one serious attempt at a model supportive residence for severely mentally ill people looks like can examine our Rising Cedars assisted living program at Touchstonemh.org
One of the cruel ironies in the way that our society deals with people suffering from schizophrenia is that we readily pay for medication regimens that can cost thousands of dollars per month, yet leave the individual with a quality of life that none of us would choose for ourselves. The implication of this alternative explanatory model of schizophrenia is that we should, instead, be spending these dollars on specially designed living environments and therapies aimed at helping them to cope with the quirks of their disordered nervous systems. Medications are certainly an important part of the treatment but it is becoming increasingly difficult to buy into the idea that “correcting chemical imbalances” is the optimal way of dealing with this major mental illness.